
Against AIDS
Sub-Saharan Africa:
Inequality - and Effective Responses - Coexist in AIDS epicenter
by Peter Lamptey, M.D. Dr.PH., President, and Rebecca Oser, M.PH, Associate Technical Officer, Institute for HIV/AIDS, Family Health International, Arlington, Va.
HIV/AIDS is likely to surpass the Black Plague as history’s most deadly pandemic: Without drastic measures, we can expect as many as 65 million deaths from AIDS over the next 10 to 15 years.
Approximately 95 percent of new infections are currently in the world's poorest countries, but HIV/AIDS knows no boundaries, has no cultural immunity, and does not spare children, killing many and orphaning more. Recently, there have been several significant, new global political and financial commitments to expand and accelerate HIV/AIDS prevention, care and treatment. These measures offer hope, but so much more must be done to quell the tide and impact of this devastating epidemic.
Understanding the Situation
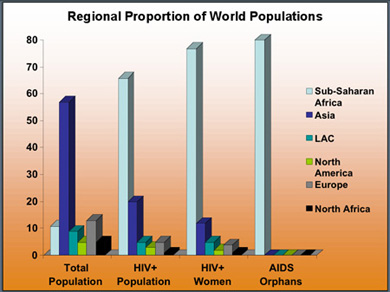
Sub-Saharan Africa has been the hardest hit region in the world: AIDS-related illnesses kill more people there than any other single cause of death. Meanwhile, an estimated 25 million people in the region are living with the virus. In 2003, 2.9 million people worldwide died from AIDS; 2.2 million, or 76 percent, of these deaths were in sub-Saharan Africa, despite the fact that the subcontinent is home to only 10 percent of the world’s population. Nearly 81 percent of the globe's 15 million AIDS-related orphans also reside in sub-Saharan Africa.
Women and adolescent girls are being infected at a particularly alarming rate. In the countries most affected by this disease, women constitute 58 percent of the HIV-positive population. They are twice as likely to be infected by a single act of unprotected sex, and girls ages 15 to 19 have rates of infection that can be 4 to 7 times higher than boys of the same age. Sexual abuse, coercion, discrimination and poverty all contribute to this inequality, as do heightened risks of stigmatization and violence for HIV-positive women.
HIV/AIDS also affects uninfected females. Women are frequently the primary care providers in a family, and many daughters and grandmothers have had to take on parenting responsibilities with very meager resources for vulnerable or orphaned children. The burden of care imposed by AIDS in a family member contributes to the further impoverishment of these women and their relatives.
Stigma and discrimination remain major obstacles in the fight against HIV/AIDS. Fear of societal disapproval restricts the freedom with which people seek information about self-protection or practice safe behaviors. Anxiety over societal ostracism also makes people resistant to voluntary HIV testing, disclosure to partners, and the use of services after diagnosis. Further, the care offered to HIV-positive people, and their perception and treatment by the community, are directly impacted by the stigma surrounding the disease.
Ensuring Program Effectiveness
In developing HIV/AIDS programs in sub-Saharan Africa, we at Family Health International (FHI) have learned that effective responses often include the following key elements:
- Bold, high-level political leadership and mobilization of international and local resources. Uganda and Botswana are excellent examples of such leadership. President Museveni of Uganda began speaking publicly about HIV/AIDS very early on. His policies of support and openness in discussing the disease helped change sexual behavior patterns in Uganda, which has aided in reducing the rate of HIV infection there significantly. In Botswana, government funding for HIV services increased, antiretroviral therapy (ART) was provided free of charge and scale-up pursued aggressively, and innovative local and international partnerships were encouraged with positive results.
- A comprehensive response consisting of: risk reduction and avoidance to prevent new HIV infections; improved access to HIV testing and counseling; prevention of mother-to-child transmission, and care for both the mother and the infant; clinical, palliative and home-based care for the ill; and support and care for affected children. For a program to be successful, it also needs to be scaled up to reach the majority of those in need – like the national initiatives in Thailand, Cambodia, Uganda and Brazil. In Thailand, for example, the prime minister unveiled a policy in 1991 requiring all sex workers to use condoms with all of their clients. Involved were the governor, chief of police and health officer for each province. Outreach included providing condoms or “health vouchers” for sex workers, and public education campaigns about the need for condom use, the dangers of unprotected or casual sex, and the legal repercussions for failure to comply with the resolution. The campaign was far-reaching and thorough, and as a result, the percentage of sex workers using condoms increased, the number of men visiting sex workers decreased, and the prevalence of HIV among sex workers and young Thai males dropped impressively.
- Prevention programs driven by epidemiology and responsive to the needs of the population at risk. Market segmentation, and targeting interventions and services to those most at risk and those in need have proved to be time-honored and sound public health approaches. For instance, risk avoidance messages such as abstinence are appropriate for delaying the onset of sexual debut in youth, while risk reduction strategies such as condom promotion and needle exchange are more suitable for sex workers and intravenous drug users.
- Involvement and ownership of HIV programming by community-based groups such as district-level governments, and nongovernmental and faith-based organizations. In each of FHI’s four focal states in Nigeria, local and state government officials, project partners, beneficiaries and other stakeholders participated in formative assessments and meetings, and assisted in designing state-level behavior change communication strategies. Participation by these groups created a sense of control and responsibility over the programs and helped ensure that they targeted the right groups, addressed issues of local concern, and used appropriate and effective language and imagery.
Going Forward
The HIV/AIDS epidemic has surged to unfathomable proportions over the past two decades. And despite tremendous strides in public awareness, political support and, more recently, access to testing and treatment, much remains to be done.
The challenges are formidable, yet we at FHI are continually impressed by the hope and faith of the people we work with, and we believe that the epidemic can be brought under control if proven interventions are implemented and sustained on a sufficiently large scale. Such an approach is the key to positive, productive impact. [back to front page....]