Center for Communications, Health and the Environment

But, Major Challenges Lie Ahead
UNICEF Reports Progress, Cites Challenges to Curtailing Global Child Mortality
In 1960, roughly 20 million newborns did not live to see their fifth birthday; by 2006, the annual number of child deaths globally fell below 10 million, to 9.7 million, for the first time since records began.
This is significant and encouraging news, yet every day on average, more than 26,000 children under the age of five still die around the world, mostly from preventable causes. Nearly all of them live in the developing world or, more precisely, in 60 developing countries. More than one-third of these children die during the first month of life, usually at home and without access to essential health services and basic commodities that might save their lives.
Born of large-scale concern, UNICEF’s landmark report, The State of the World’s Children 2008, examines the status of child survival and primary health care for children across the globe, with a strong emphasis on trends in child mortality. This seminal report by the United Nations Children’s Fund (UNICEF) outlines the results of long-term partnerships developed in response to the child survival revolution, reviews the experiences and approaches to child survival and health of recent decades, and appraises the lessons from failures and successes in child survival over the past century.

The centerpiece of the report examines several of the most promising approaches – community partnerships, the continuum of care framework and health-system strengthening for outcomes – to reach those mothers, newborns and children who are currently excluded from essential interventions. By highlighting examples from countries and districts where these have been successful and exploring the main challenges to their expansion, this report offers practical ways to jump-start progress.
The Current State of Child Survival, Mortality and Health
The State of the World’s Children 2008 documents impressive progress since 1990 in improving the survival rates and health of children, even in some of the world’s poorest countries. In fact, the global child mortality rate declined by almost 25 percent between 1990 and 2006 (the most recent year for which firm estimates are available). Meanwhile, increased coverage of measles vaccinations and follow-up campaigns, for example, contributed to a 60 percent fall in global measles deaths and a 75 percent reduction in measles mortality in sub-Saharan Africa between 1999 and 2005. Recent years have seen important and, in some cases, remarkable advances in child survival, despite considerable impediments, most notably the onslaught of AIDS in Eastern and Southern Africa, and internecine conflict in many high-mortality countries.
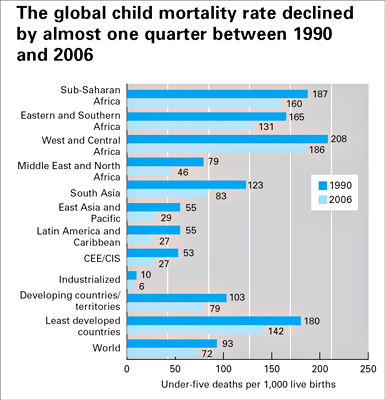
Looking at the overall picture, in 2006, the global child mortality rate was estimated at 72 deaths per 1,000 live births, 23 percent lower than the 1990 level. Child mortality rates have been roughly halved in East Asia and the Pacific; Central and Eastern Europe and the Commonwealth of Independent States (CEE/CIS); and Latin America and the Caribbean – bringing the under-five mortality rate for each of these regions below 30 per 1,000 live births in 2006. (The average rate of industrialized countries in 2006 was six deaths per 1,000 live births.)
The Middle East and North Africa region also has seen steady progress in reducing rates. South Asia is making headway as well, although it still has the second highest number of child deaths, accounting for 32 percent of global under-five mortality rates, with undernutrition a major contributing factor.
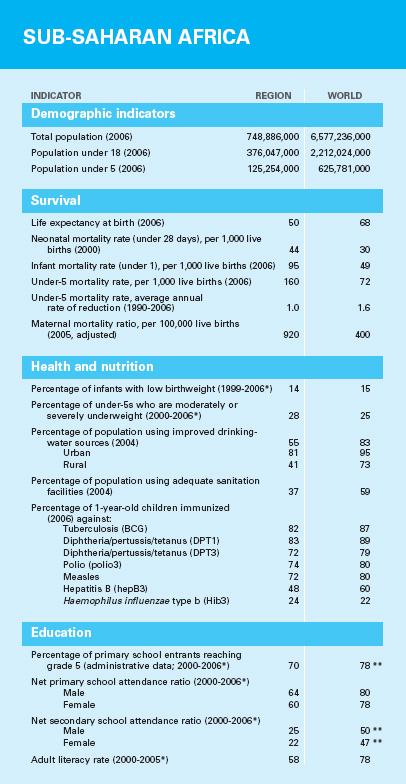
Sub-Saharan Africa remains the most troubling geographic area. It has the highest rate of child mortality by far: On average, one in every six children there dies before age five. In addition, the region as a whole has shown the least progress, managing to reduce the burden of child mortality by only 14 percent between 1990 and 2006, with a number of countries in the region registering increases in under-five mortality rates. In 2006, 49 percent of all deaths of children under age five occurred in sub-Saharan Africa, despite the fact that only 22 percent of the world’s children are born there.
Reducing Under-Five Mortality—Achieving Millennium Development Goal 4
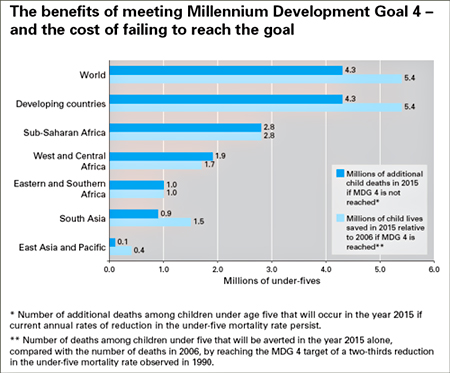
The current focus of the development community in relation to child survival is Millennium Development Goal (MDG) 4, which aims to reduce the global rate of under-five mortality by two-thirds between 1990 and 2015. At present, four regions are on track to meet MDG 4: East Asia and the Pacific; Latin America and the Caribbean; CEE/CIS; and the industrialized countries/territories. Despite recent progress, achieving this goal will require a reduction in the number of child deaths between 2008 and 2015 at a far faster rate than the world has managed since 1990. If current trends continue, 4.3 million child deaths will occur in 2015 that could have been averted had MDG 4 been met.
On a country-by-country basis, UNICEF estimates that 129 nations are on track. Some of these have already met the 2015 goal for reducing child mortality, while others are poised to do so. Approximately 18 percent, or 35 countries, are making progress towards achieving MDG 4, but at a rate that is insufficient to meet it in full and on time.
Of most concern are the 27 countries that have registered scant progress since 1990 or have an under-five mortality rate that is stagnant or higher than it was 18 years ago. Of the 46 countries in sub-Saharan Africa, for example, only Cape Verde, Eritrea and Seychelles are on track to meet MDG 4. The region as a whole only managed to reduce child mortality at an average annual rate of 1 percent from 1990 to 2006, and double-digit reductions will be needed during each of the remaining years if it is to meet MDG 4.
MDGs Prioritize Children
In addition to MDG 4, curtailing child mortality especially requires reducing poverty and hunger (MDG 1), improving maternal health (MDG 5), combating HIV, AIDS, malaria and other major diseases (MDG 6), and improving water and sanitation (MDG 7).

Improving maternal and child nutrition is, in fact, a prerequisite for achieving MDG 4. Seemingly simple things like upping the developing world’s consumption of iodized salt, making sure more infants are exclusively breastfed during their first six months of life, and ensuring a full, two-dose coverage of vitamin A supplementation worldwide would go a long way towards achieving this goal. Meanwhile, almost 40 percent of all under-five deaths occur during the first 28 days of life from complications, including poor maternal health and care. In fact, one in every four pregnant women in the developing world receives no antenatal care, according to the latest estimates for 2000–2006, and more than 40 percent give birth without the assistance of a skilled attendant. Each year, more than 500,000 women die in childbirth or from complications during pregnancy, a probable death sentence for their babies.
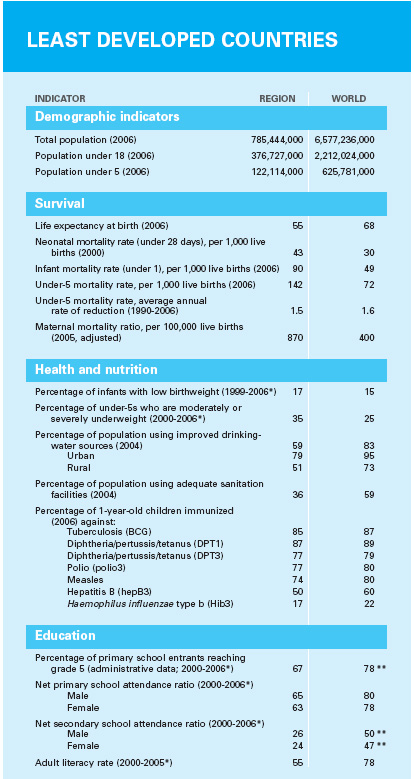
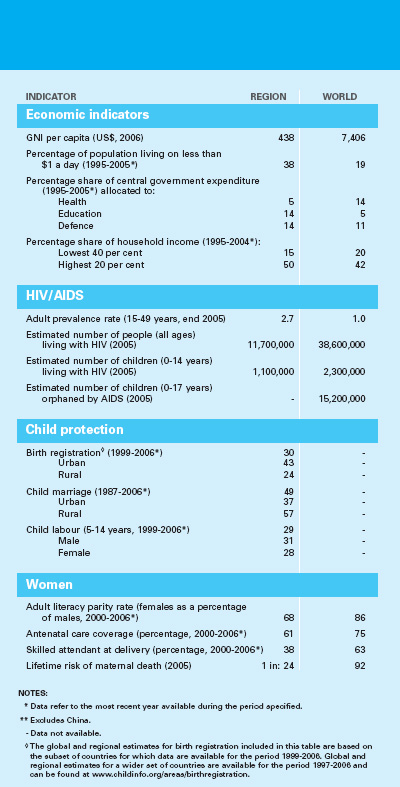
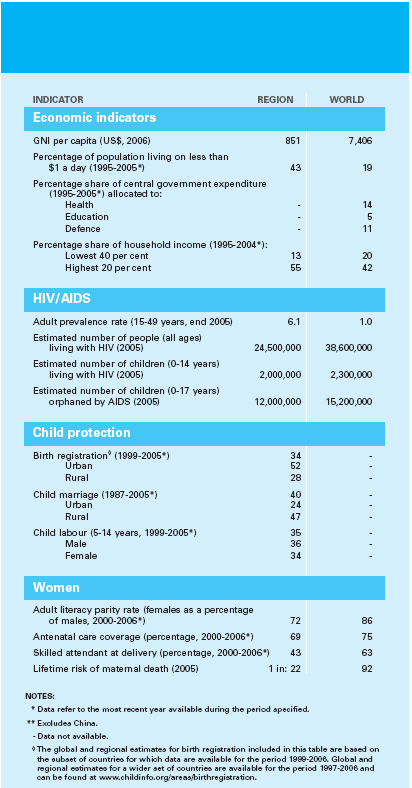
As if that’s not punishment enough, half of the infants infected with HIV will die before age two; malaria accounts for 8 percent of deaths in children under five; and measles for another 4 percent. Worldwide, 2.3 million children under age 15 are living with HIV, mostly in sub-Saharan Africa, and 530,000 children were newly infected with the virus in 2006, mostly through mother-to-child transmission. And while the world as a whole is on track to meet the MDG target for safe water, insufficient progress towards improved sanitation is making it difficult to combat diarrhea, which currently kills almost 2 million children every year.
Setting Priorities to Achieve MDGs and Improve Child Survival
The key interventions needed to address the major causes of child deaths are well established and accepted. In fact, research reveals that only about 1 percent of deaths among children under five have unknown causes and that two-thirds of them are entirely preventable through basic, yet important, services and practices such as having skilled attendants involved in delivery and newborn care; hygiene promotion; adequate nutrition; micronutrient supplementation to boost immune systems; oral rehydration therapy and zinc to combat diarrheal disease; and antibiotics to fight pneumonia.
Although much has been achieved to date, implementing these and other solutions has proved far more arduous than experts predicted at the start of the child survival revolution, and the results have been more elusive. In response, the development community is increasingly coalescing around priorities, which could provide the impetus needed to implement these basic services and practices, and achieve the health-related MDGs. These priorities include:
- Focusing on 60 countries where the burden of child mortality is highest, and which in 2005 together accounted for 93 percent of all under-five deaths.
- Providing a continuum of care for mothers, newborns and children by packaging interventions for delivery at key points in the life cycle.
- Strengthening community partnerships and health systems.
Evolving Health-Care Systems and Practices
The main challenge to child survival no longer lies in determining the proximate causes of or solutions to child mortality, but in ensuring that the services and education required for these solutions reach the most marginalized countries and communities.

Effective scale-up requires that we learn from the lessons of recent decades – with a particular emphasis on strengthening integrated approaches to child health at the community level. The current dominant framework for integration is the Integrated Management of Childhood Illness (IMCI), the strategies of which more than 100 countries have adopted since their 1992 introduction and which aim to improve health worker performance, strengthen health systems, and enhance community and family practices. Meanwhile, the more recent Accelerated Child Survival and Development initiative concentrates on community-based promotion of family health, nutrition and hygiene practices; outreach efforts and campaigns to provide essential services and products; and facility-based delivery of an integrated minimum-care package. It now covers more than 16 million people in 11 countries that have high rates of under-five mortality and builds on the strengths of existing approaches, including IMCI and the Expanded Programme on Immunization, which launched in 1974 and has been the most successful public health program to date.
In pursuing effective scale-up, interventions must be provided –- and initiatives developed –- within a continuum of care that engages communities and households, as well as outreach and facility-based care. Health systems must be strengthened at all levels and expanded to support new initiatives, including community partnerships, and they must be backed by strong national and international leadership and commitment. In addition, the many institutions involved in maternal and child survival, health and nutrition must work together effectively.
The projected impact of achieving a high rate of coverage with a continuum of health care could be profound. In sub-Saharan Africa, for example, achieving a continuum of care that covered 90 percent of mothers and newborns could avert two-thirds of newborn deaths, saving 800,000 lives each year.
Strengthening Community Partnerships and Health Systems
Community partnerships and participation show great potential to improve health, nutrition and environmental conditions, especially in countries with low health-system capacity, and particularly for the most marginalized and the poorest populations. Experience shows that successful community partnerships are based on several common factors:
- Cohesive, inclusive community organization and participation: Programs that build on established structures within a community, are socially inclusive and include community members in the planning, evaluation and implementation are among the most successful in developing countries.
- Support and incentives for community health workers: As primary agents of community-based treatment, education and counseling, these individuals require acknowledgement and encouragement to prevent attrition, meet their obligations and sustain motivation.
- Adequate program supervision and support: Supervision is required to sustain community members’ interest and motivation, and lower the risk of attrition; support includes logistics, supplies and equipment.
- Effective referral systems to facility-based care: Hospitals and clinics are essential complements to successful community partnerships, providing services that cannot be safely replicated elsewhere; district health systems also serve as a focal point for public health program coordination.
- Cooperation and coordination with other programs and sectors: An integrated approach to maternal, newborn and child health necessitates collaborative action between programs and sectors addressing health, nutrition, hygiene, major diseases and food security, as well as intersectoral collaboration to address transportation infrastructure and access to water and sanitation facilities.
- Secure financing: To be successful over the longer term, financing for community partnerships should address considerations of sustainability and equity, including such issues as cost-sharing and financial incentives for community health workers.
- Integration with district and national programs and policies: Consultative multi-stakeholder processes are needed to develop strategies and ensure that maternal and child survival feature prominently in national and decentralized plans and budgets, with clear goals and concrete benchmarks.

There are numerous examples of successful community partnerships in primary health care for mothers and children in CEE/CIS; East Asia and the Pacific; Latin America and the Caribbean; the Middle East and North Africa; South Asia; and, increasingly, in sub-Saharan Africa. Some community-based health programs are small-scale, involving only a few thousand or even a few hundred people; other initiatives, such as the Brazilian community health workers network or the Lady Health Workers program in Pakistan, encompass thousands of workers covering millions of children and women. The challenge is to learn from these experiences, take the programs to scale and reach the millions whom the health system continues to pass by.
In addition, national leadership and ownership of community partnerships are essential to ensure sustainability and foster expansion. Governments have a critical role in developing and implementing policies to lower barriers to primary health care, improving the quality and efficiency of service providers, and increasing public accountability.
Based on the joint framework developed by leading international agencies, including the World Bank, the World Health Organization and UNICEF, The State of the World’s Children 2008 has identified five distinct yet related actions to building up health systems across developing countries and territories through programs, policies and partnerships during the coming decade:
Action I: Realign programs from disease-specific interventions to evidence-based, high-impact, integrated intervention packages to ensure a continuum of care.
Action II: Make maternal and child health a central tenet of integrated national planning processes for scaling up essential services.
Action III: Improve the quality and consistency of financing for health-system strengthening.
Action IV: Obtain national political commitment.
Action V: Create conditions for greater harmonization of global health programs and partnerships.
Uniting for Child Survival
For governments, donors, international agencies and global health partnerships, effective scale-up will require a new way of working in primary health care among the key stakeholders. The central theme of this paradigm is unity. Initiatives and partnerships directed towards improving aspects of maternal and child health abound and continue to proliferate, but they will require greater coherence and harmonization to meet the health-related Millennium Development Goals for mothers and children.
The MDGs represent our best hope to accelerate human progress. Achieving the goals will mean that the lives of around 30 million children and 2 million mothers will have been spared between 2005 and 2015. Meeting the objectives will also result in hundreds of millions of children, men and women being relieved of hunger, utilizing safe water and basic sanitation, obtaining an education, and enjoying the same economic advantages and political opportunities that are available to others. The MDGs may also foster more balanced population dynamics, since, when parents are convinced that their children will survive, they are more likely to have fewer children and provide better care to those they have – and countries can invest more in each child.
Although several regions and nations are lagging, the targets are all reachable in time if the political will, necessary resources and required strategies are put in place. Six pivotal actions urgently need a unified response:
- Create a supportive environment for maternal, newborn and child survival and health by ensuring that health systems and programs are rights-based – and by supporting peace, security, child protection, non-discrimination, gender equality and the empowerment of women.
- Develop and strengthen the continuum of care across time and location. The continuum must deliver essential services at key points during the life cycle of mothers and children. Strong links are also required between the household, the community, and quality outreach and clinical services at primary health facilities and district hospitals.
- Scale up packages of essential services by strengthening health systems and community partnerships through initiatives to train health workers, extend outreach services, overcome bottlenecks and exploit new technologies.
- Expand the data, research and evidence base. Although the evidence base on maternal and child health is being provided by a rich array of resources, there is still a demand for more rigorous data collection and dissemination, research and evaluation.
- Leverage resources for mothers, newborns and children. Donor assistance is rising, but not fast enough to meet the goals. National governments must also fulfill promises to boost health spending.
- Make maternal, newborn and child survival a global imperative.
Accelerating progress will necessitate positioning these objectives at the heart of the international agenda in the run-up to the 2015 deadline for the Millennium Development Goals. The challenge is to build on the progress achieved across the developing world, particularly during recent years, in preventive interventions delivered by outreach services.
The foundation for action – built on data, research and evaluation – is well established. The frameworks – community partnerships, the continuum of care and health-system strengthening for outcomes – are well defined. In effect, the means are in our hands. It is now a question of will, urgency and action.
The State of the World's Children 2008 is UNICEF's landmark report in the struggle to reduce childhood mortality. The above synopsis of the report includes excerpts, highlights and information on UNICEF’s Millennium Development Goals, which were adopted by world leaders in 2000 and focus on children.world.
Click here to read: Lead Article | Q&A | CECHE News

Dr. Sushma Palmer, Program Director
Valeska Stupak, Editorial & Design Consultant
Shiraz Mahyera, Systems Manager
Rohit Tote, Website Consultant